Patient Centered Medical Home (PCMH) embodies the current trajectory of healthcare in that the patient is the focus of the medical model. The National Committee for Quality Assurance’s (NCQA) PCMH program is vastly adopted, with more than 12,000 practices, 60,000 clinicians, and 100 payors participating. In fact, 1 in 6 eligible physicians in the U.S. practices in an NCQA-Recognized PCMH.
With the objective to strengthen patient-provider relationships, reduce healthcare costs, and improve quality, NCQA continues to accelerate the growth of value-based care with the remodel of their PCMH program. Changes to the new PCMH model reduces the burden of the reporting process and focuses on increased healthcare quality and practice performance.
Redesigned reporting process and criteria
The redesigned PCMH program is effective September 30th, 2017 and practices that plan to get recognition using the 2014 standards must do so before then. Most notably, “once the practice has been recognized as a medical home, it will never have to renew its application from start to finish,” explained Michael Barr, MD—executive vice president of the organization’s quality measurement and research group—in a recent Medical Economics article detailing the changes.
In addition to the ongoing recognition status, reporting is moving from a three-year cycle to an annual online “check-in” with a dedicated NCQA point of contact. Fortunately, screenshots and egregious written documentation is reduced in the new redesign. Online interaction, facilitated through a screen-sharing session, and data submission is now the method that practices employ to prove they are meeting core requirements.
Out of the 17% of primary care practices in the U.S. that wield NCQA’s PCMH badge, 75% of them are recognized as PCMH level 3. To demonstrate the majority of level 3 practices, the new recognition structure is flattened to a single level. Vice President of Product Design and Support, Patricia Barrett explains that the change will enable “a much clearer delineation between practices that are recognized by the NCQA and those that aren’t.”
[INFOGRAPHIC] 8 Referral Management Stats You Need to Know:

Increased patient satisfaction and financial reward
The origin of practice transformation for many medical homes revolves around highly collaborative provider relationships for improved patient care.
According to a Hartford Foundation Study, 83% of patients said that being treated in a PCMH improved their health1.
In addition to improved health, patients are more satisfied with urgent appointment scheduling. In a study published in Becker’s Hospital review, patient satisfaction increased from 12 percent to 53 percent in a PCMH practice, while in the control clinics the scores improved from 14 percent to 18 percent2.
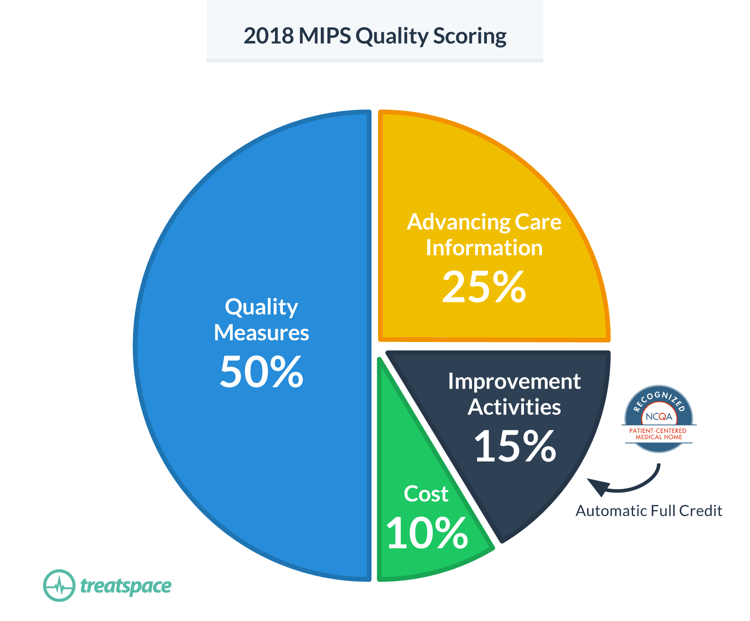
Redesigned PCMH guidelines are preparing practices for prospective models of payment that incentivize patient-centered care. According to the NCQA Toolkit, available for download on their website, “becoming an NCQA-Recognized PCMH or PCSP directly increases clinician payments through the Merit-Based Incentive Payment System (MIPS).” Improvement Activities account for 20% of a practice’s MIPS score (15% in 2018) under MACRA and as a NCQA-Recognized PCMH or PCSP that practice will receive automatic full credit in the category.
“...becoming an NCQA-Recognized PCMH or PCSP directly increases clinician payments through the Merit-Based Incentive Payment System (MIPS).”
The other 3 categories contributing to MIPS; Quality Measures, Advancing Care Information, and Cost (2018), will likely be met by PCMH practices. Measures set forth in the recognition program that improve coordination of care, promote the use of health information technology (HIT), and improve patient outcomes overlap with MIPS requirements.
Finally, more than 100 payors are offering financial incentives to practices operating within the PCMH framework. Accredited practices must “seek out value-based contracts to fully capitalize on the transformation,” as encouraged by MGMA3. In the same article, Steven Blubaugh of DHG Healthcare explains that practices “risk missing out on very important revenue by not asking commercial payers to increase their reimbursement due to improved care delivery.”
[FEATURED EBOOK] A Primary Care Leader's Journey to Value-Based Care
Treatspace helps practices meet PCMH guidelines
Within the new redesign, practices must meet 40 core criteria and 60 elective criteria (down from 167 in 2014’s program), which are organized into six concepts:
- TEAM-BASED CARE AND PRACTICE ORGANIZATION (TC)
- KNOWING AND MANAGING YOUR PATIENTS (KM)
- PATIENT-CENTERED ACCESS AND CONTINUITY (AC)
- CARE MANAGEMENT AND SUPPORT (CM)
- CARE COORDINATION AND CARE TRANSITIONS (CC) - Treatspace actively meets
- PERFORMANCE MEASUREMENT AND QUALITY IMPROVEMENT (QI)
Practices must receive 25 points within five of the six above groups in order to qualify as a PCMH.
Treatspace helps practices meet several measures of the fifth competency: Care Coordination and Care Transitions (CC). NCQA describes attesting to CC as a practice that “systematically tracks tests, referrals and care transitions to achieve high quality care coordination, lower costs, improve patient safety and ensure effective communication with specialists and other providers in the medical neighborhood.”
Utilizing dashboards from previous PCMH applications, we’ve identified several competencies of the new PCMH model that Treatspace continues to support.
CC 04 (Core): The practice systematically manages referrals by:
- Giving the consultant or specialist the clinical question, the required timing and the type of referral.
- Giving the consultant or specialist pertinent demographic and clinical data, including test results and the current care plan.
- Tracking referrals until the consultant or specialist’s report is available, flagging and following up on overdue reports.
Preferred specialists only receive patient referrals that are covered with the insurance they accept. Providers can choose to attach last office visit notes (OVNs), clinical data, and demographic information. In addition, they can customize they test results they want to send along with the referral. Care coordinators can track patients, identify gaps in care, and manage the status of referrals from a centralized dashboard.
CC 06 (1 Credit): Identifies the specialists/specialty types frequently used by the practice.
Practice leadership utilizes referral performance analytics to gain a comprehensive view of their practice’s referral patterns. Segmenting data by provider and practice level allows primary care to view which specialties and individual specialists they refer to most often.
CC 07 (2 Credits): Considers available performance information on consultants/specialists when making referrals.
Treatspace provides primary care with report card views of each specialist within their network so they can monitor consult report compliance, time to treatment, and time to acceptance. Specialist performance metrics are taken into consideration during referral decision support process and allow practice executives to make narrowed network decisions in line with payor contracts and value-based programs.
CC 11 (1 Credit): Monitors the timeliness and quality of the referral response.
Referral analytics track referral volume, average time to accept a referral, and average time to see a patient.
CC 12 (1 Credit): Documents co-management arrangements in the patient’s medical record.
Treatspace enables your practice to work with preferred partners to develop care compacts that are measured and tracked within the platform.
CC 21 (Maximum 3 Credits): Demonstrates electronic exchange of information with external entities, agencies and registries (May select one or more):
- Regional health information organization or other health information exchange source that enhances the practice’s ability to manage complex patients. (1 Credit)
- Immunization registries or immunization information systems. (1 Credit)
- Summary of care record to another provider or care facility for care transitions. (1 Credit)
All referrals pass seamlessly from a practice’s EHR to their preferred specialist partner through Treatspace. Transition of Care (TOC) documents have the ability to auto-attach to referrals to improve workflow and save time. The Direct addresses of all specialists are no longer required and each transaction is easily accessible in a cloud-based log.
In conclusion, Patient Centered Medical Homes continue to improve patient care by transforming how primary care is organized and delivered. Newly implemented guidelines make reporting and documentation easier on practices so they can focus on providing the highest quality of care to their patient population. What are some of the changes that your practice is most excited about? Share in the comments below.
[DOWNLOAD EBOOK] A Primary Care Leader's Journey to Value-Based Care
1) Hartford Foundation | Transforming Primary Care What Medicare Beneficiaries Want and Need from Patient-Centered Medical Homes to Improve Health and Lower Cost
2) Beckers Hospital Review | http://www.beckershospitalreview.com/hospital-physician-relationships/study-pcmh-model-improves-patient-satisfaction.html
3) MGMA | http://www.mgma.com/practice-resources/mgma-connection-plus/online-only/2017/march/making-your-pcmh-transformation-a-success-step-by-step